Virtual Reality and Eating Disorders: Why Should We Bring Virtual Reality Therapy to Kentucky?3/9/2018 Virtual Reality and Eating Disorders: Why Should We Bring VR Therapy to Kentucky?
By: Lisa Michelson Within recent years, virtual reality has gained popularity in the entertainment industry. This new domain, where entertainment and technology intersect, has transformed games and television, making a whole new experience for the user. Healthcare providers have also noticed, and have begun to take advantage of this whole new world of possibilities for treating their patients. Here are a few examples of how health professionals, specifically mental health professionals have begun using virtual reality (VR). VR has been used to treat phobias, anxieties, and fears (Garcia-Palacios et al., 2002). In the United States, Duke University has used VR as a form of cognitive behavioral therapy (CBT) for individuals with anxiety disorders (Zielinski et al., 2006). At the University of Southern California, a VR exposure therapy has been developed in order to address PTSD symptoms for individuals returning from military service in Iraq and Afghanistan (Rizzo & Hartholt, 2005). There are VR medical centers, VR clinical trials, and therapies that continue to be developed. In the eating disorder field, virtual reality is being used to implement CBT for individuals who suffer from eating disorder (ED) behaviors and symptoms. The kinds of VR experiences can range from a full body emersion (wearing sensors all over one’s body) to wearing goggles (for the user to see the VR world they have been placed in). Below is a list of some VR scenarios that participants have been placed in for treatment in Bulimia Nervosa (BN) and Binge Eating Disorder (BED) (Regine de Carvalho et al., 2017):
Furthermore, below is a list of some outcomes that have been observed in utilizing VR in ED treatment (Regine de Carvalho et al., 2017):
Although Regine de Carvalho et al. (2017) did a systematic review of VR in the assessment and treatment of BN and BED, the number of studies that utilized VR in the treatment of BN and BED is few. In researching the use of VR in treating Anorexia Nervosa (AN), the number of studies that used VR within the United States was practically non-existent; most of AN and VR research being conducted in Europe, specifically Spain and Italy (Riva et al., 1999; Perpina et al., 1999). In the previously mentioned studies, utilizing VR in ED treatment has been shown to improve behaviors and symptoms in participants. In other words, what is being done in these treatments IS working. However, the use of VR as exposure therapy for eating disorder treatment is still not only infrequently used, but underutilized and underdeveloped in the United States. Here, at the EAT Lab, one of my jobs has been to find collaborators and programmers to develop such technology. While it has been a steep learning curve in understanding what technology would be most user-friendly, financially reasonable, and the best for therapy, we continue to learn more about this technology every week. In our own research into VR software development, it has become apparent why this form of therapy rarely exists in the United States; the combination of technology/entertainment and mental health therapy is still an unchartered (yet exciting!) territory. Communicating the wants/needs of what we, the therapists, want in the VR technology to the software development is like talking between two languages. However, through talking with multiple resources, we have hope that we are closer to brining this technology to Louisville and being amongst the first ED research facilities here to provide this cutting edge therapy to our clients. To address the question that was posed in the title of this article (Why Should We Bring VR Therapy to Kentucky?), we know it can work to improve health outcomes for our clients and we hope that future advancements will provide more insight to our exposure therapy research.
3 Comments
Fighting the Stigma, Increasing Awareness and Education: Advocating for Eating Disorders in Kentucky2/6/2018 Fighting the stigma, increasing awareness and education: Advocating for eating disorders in Kentucky
By Leigh C. Brosof Fighting stigma, increasing awareness, and educating our communities about eating disorders are essential for early detection and treatment of these disorders; and we know that the earlier we catch an eating disorder, the more likely an individual is likely to recover. In the state of Kentucky, there is no officially recognized awareness efforts or state-sponsored educational programs about eating disorders. That is why today (February 5, 2018), myself, Dr. Levinson, and Melissa Cahill, an eating disorder advocate in Louisville, traveled to Frankfort, KY to meet with our legislators to discuss how we can get the state involved in the fight against eating disorders. We had meetings with Representative Ken Fleming, who is also the executive director of the Kilgore Counseling Center, and Senator Ernie Harris about sponsoring a resolution in the Kentucky House of Representatives and Senate, respectively, to officially recognize February 26-March 4th as Eating Disorder Awareness Week in the state of Kentucky. We also spoke with them about what other states have done to further the cause of supporting eating disorder awareness. In Missouri, the local government created an eating disorder coalition dedicated to awareness and providing education to health providers about treatment standards. In Pennsylvania, the legislature passed a bill requiring all middle and high schools to provide a fact sheet on eating disorder detection and what to do if you think someone has an eating disorder. These efforts show that state support really can make a difference in the fight against eating disorders, and we hope that Kentucky will follow these examples. Indeed, in addition to meeting with Representative Fleming and Senator Harris about the resolution, we also asked about longer-term plans to get legislation passed in order to increase awareness and education about eating disorders in Kentucky. Both were immensely supportive in helping us understand the steps in order to get such a bill developed. We were briefly introduced to Representative Kimberly Moser and Senator Julie Raque Adams, who both serve on the Health and Welfare Committee, through which the legislation would be drafted. Our ultimate goal is to see a coalition created similar to the one in Missouri: one that spreads awareness and education, provides training to health care providers in eating disorder care, and establishes treatment recommendation guidelines for best care. In the meantime, we are thrilled to see that our legislators are listening to the need for state support of eating disorders in Kentucky and to recognize Eating Disorder Awareness Week, which will be the first piece of legislation including eating disorders ever passed (hopefully) in the state. We are also excited to continue to advocate for eating disorder awareness in Kentucky. Overall, it was a fun and encouraging day, and we are grateful to our legislators for taking the time out of their day to meet with us. This was my first experience with formal advocacy work with legislators, and I look forward to continuing to work toward our goals. But it’s also important to remember that advocacy takes many forms, and it doesn’t always take a trip to Frankfort to make a real difference. Post on social media. Attend a walk. Put posters up around a school or work building. Bring in a speaker or attend a lecture. That’s all it takes to start advocating for eating disorder awareness in our community. Louisville has come such a long way in the short time I’ve been here, and I’m excited to see how we can advocate for a better future for every individual with a diagnosis of an eating disorder. Avoidance versus Exposure: The Importance of Facing Your Fears
By Caroline Christian What are you afraid of? We are all afraid of something. Fear is not only normal, it is healthy! The tinge of fear you get when a large blur crosses your periphery when you are walking in the woods is the same fear that has kept humans alive for hundreds of thousands of years. Fear helps us to recognize and escape when we are in dangerous situations. The problem with fear is that we can become afraid of things that can’t really hurt us, such as taking a test, giving a presentation, or eating certain foods. These fears may stop us from doing things we like to do or from having meaningful relationships, potentially spiraling into more stress, anxiety, and even isolation. The good news is that there are things we can do to reduce these fears. There are basically two options: you can avoid the thing you fear or you can face the fear head on. To see these two strategies in action, let’s look at an example. Say you are afraid of talking to new people: 1) You can avoid putting yourself in a situation where you may have to talk to new people. This would likely mean avoiding grocery stores, job interviews, dating, holiday parties, traveling, doctors’ appointments, etc. The benefit of this is that never facing your fear can provide a brief sense of relief, and may lessen your anxiety in the short term because the fear is not imminent. However, the problem with this method is that avoidance can intensify the fear in the long term, because by never experiencing this irrational fear, you never see that it isn’t as bad as you thought it would be. 2) Or you can actively put yourself in situations where you will have to talk to new people. This could be something like: initiating small talk with a new coworker, asking someone on a date, complimenting a stranger at the store, hosting a party, etc. The downside of exposing yourself to your fear is that it can be difficult at first and may cause some (or a lot of!) anxiety. However, the benefit is that by facing the thing you are afraid of, you get to see that you are strong enough to handle it. Over time if you continue to expose yourself to that fear, the anxiety will lessen and the fear will have less control over your life. Thus, when it comes to handling fear it may be easier initially just to avoid it, but avoidance in the long-term only serves to worsen the fear. Exposure has the opposite effect: while it may be difficult initially, repeated exposures can lessen the anxiety and make it more bearable. This idea is the basis of exposure therapy, which is a cognitive-behavioral approach that has been shown to be effective in treating anxiety disorders, including specific phobias, PTSD, and OCD. Exposure allows people to confront their fears in a safe and controlled environment, so that when the fears come up in the real world, they have less anxiety and are equipped with the tools to handle it. In contrast to the many clinicians that utilize exposure to treat anxiety and eating disorders, there are a small number of psychologists that advocate for avoidance methods in therapy. This approach has been spurred by the increased awareness of using politically correct language and avoiding triggering words in our society. Topics that are controversial, or that could be potentially painful for individuals based on their past experiences, typically are avoided in academic or professional settings. Although it may be helpful in some places in our society, this type of avoidance does not have a place in therapy or rehabilitation programs. The problem with avoidance in therapy is the same as avoidance in the real world. By never experiencing the fear, you never see that it isn’t as scary as you imagined. This will cause the anxiety to build up, and then if something happens to trigger these emotions outside of therapy, the anxiety will be even worse. That is why exposure is so important in therapy- talking about things that are scary and anxiety provoking in a safe environment allows for less anxiety when faced in the real world. Additionally, there are things you can do outside of therapy to implement these strategies to better your own life. Beyond therapy, exposure also can be used to tackle everyday anxieties, like testing anxiety or public speaking. Taking sample tests, practicing with friends and coworkers, and visualization exercises are all exposure-based techniques that can help reduce tension and anxiety, so it doesn’t build up on the big day. So in conclusion, when it comes to battling your fears (whether they are big or small) choose exposure! Although it is difficult at first, in the long term it will give you more control over your fears. In the EAT lab, we are exploring the use of exposure therapy for eating disorders by exposing people to fears such as gaining weight, losing control, making mistakes, or eating certain foods. If you struggle with an eating disorder and you are interested in participating in these studies, click here! Additional reading: This article discusses ways in which we use avoidance in every day life, and may not even realize it! Check out this article on how to implement exposure strategies into your everyday routine.  Reflections from ABCT 2017
By: Cheri A. Levinson, Ph.D. The EAT lab (pictured to the right) just returned from ABCT 2017 in San Diego, California. To say that this conference was inspiring would be an understatement. I think the entire lab left the conference feeling renewed and excited about all of the immerging research both within the eating disorder field and in clinical psychology as a whole. Here are a few highlights from our trip. Exposure in eating disorders. There was not one, but *two* symposiums focused on using exposure therapy to treat eating disorders. Given this area has been my passion for more than half of my career (which admittedly has not been that long yet), I am excited to see not only more work on the topic, but a growing interest and excitement within the eating disorder field. There were two talks that especially stood out to me on the impact they can bring to the field. First, Nick Farrell (from Rogers) presented work from his partial hospital program showing how exposure and response prevention can be integrated into a partial program. Second, Jamal Essayli (from Penn State Hershey) began to answer the question ‘Can we use exposure therapy during refeeding?’ The answer seems to be a resounding yes. Food exposure does not cause harm and in fact decreases anxiety around food during refeeding. Some research has proposed that we need to wait to use food expose with eating disorder patients until they are weight restored (e.g., instead of getting them to eat while distracting etc), since exposing them to food does in fact lead to their feared concern of weight gain. This research suggests that no, programs should go ahead and start using exposure even when patients are underweight. Personalizing Treatment. I was lucky to be part of a fantastic symposium including Aaron Fisher (Berkley), Eiko Fried (U Amsterdam), Anne Roefs (Maastricht U), Sarah Jo David (Texas Tech), and Rich McNally (Harvard) that focused on using network analysis to personalize treatment. We got to hear about how network analysis is being used to lead to personalized treatment of anxiety, depression, eating disorders, and obesity. We also got to learn a bit about how we might use machine-learning to predict behaviors such as smoking. The main take away from this symposium, in my mind, is that technology is taking us to new places where we don’t have to rely on averages and can use data to make each treatment plan the best possible for each person. Graduated Exposure versus Using a Hierarchy. Work from Ryan Jacoby at Mass General suggests that we don’t necessarily need to use an exposure hierarchy to treat OCD/anxiety. Instead, we can randomly choose exposures (regardless of difficulty level) and that this method may in fact maximize intolerance of uncertainty and produce better change (and surprisingly less drop out!). Push for Open Science. One of the undertones of the conference was a push for Open Science. I have to give credit to Aaron Fisher for his plea during the personalized network symposium encouraging researchers to share their data. The message that I took away is that the more we collaborate and are open about our science, the more likely we are to really help people. Overall, I felt inspired by the amount of collaboration and willingness of our colleagues to be open and work toward creating science that can have real impact. Thanks ABCT for another great conference- already looking forward to next year! Eating Disorders Impact People of All Ages
by: Lisa Michelson, M.A. Eating disorders happen at every age. From preteens to older adults, eating disorders do not discriminate. Previously, there was a long-held view that eating disorders are mental illnesses that mainly affect adolescents and young adults (e.g., Bruch, 1973). Subsequently, much of the eating disorder research has focused on these age groups (Rohde et al., 2015; Allen et al., 2014). However, as instances of eating disorders in older individuals increased, which may be attributed by an increase in awareness rather than an overall increase in eating disorders in older individuals, there became a need to treat this population as well. Unfortunately, eating disorders continue to be poorly understood in middle age and older populations. The comparison between how eating disorders manifest in older adults versus younger adults is even more elusive. As we have begun to understand more about eating disorders, we have learned that fears and symptoms manifest in a variety of ages and also in a variety of ways. For example, at the onset of menopause, women may begin to alter how they view their body, which can lead to an increase in one’s body dissatisfaction (Gupta, 1990; Peat et al., 2008). In other words, as a woman’s body begins to change due to a decrease in hormonal production, she may become dissatisfied with how she experiences her body. Conversely, we see body dissatisfaction in younger women may result from media portrayals of the “ideal” female body and femininity (Tiggemann & Stevens, 1999). Granted, older women are also affected by media portrayal of older women, but not to the same degree as younger women. In comparing the two ages, Rand and Wright (2000) found that older women have more realistic cognitive perceptions of their bodies. This literature may provide insight as to why older women are less affected by external factors (i.e. cultural factors) compared to younger women. Thus, it seems plausible that these cognitive, biological, and cultural differences may also manifest in different core fears in eating disorders in younger versus older individuals. So why is this important? Why is identifying the differences between ages necessary? Therapy improves health outcomes for individuals of all ages in treatment for ED behaviors and fears. Furthermore, it is crucial to understand how etiological differences in various ages may contribute to diverse therapy outcomes. In other words, to treat a younger individual with AN in the same manner as an older individual with AN may lack efficacy. Yes, they both suffer from the same disorder; however, the reasons for engaging in such behaviors may be vastly different. It would be like a mechanic expecting to fix two cars in the same way. Age may differentially influence how fears impact eating disorder symptoms. In a recent study, we analyzed if age moderated the relationship between the eating disorder symptoms and fear of food. Yes! We found that age moderated the relationship between fear of food and eating disorder symptoms (come see us present this work at ABCT!). Specifically, we found that fear of food is more related to eating disorder symptoms in younger versus older participants. What does this mean? Older participants and younger participants differ in how food-related anxiety impacts eating disorder symptoms. This specific type of fear (food) may be most relevant in younger adults. This means we still need to figure out what types of eating-related fears are most relevant in older age! It is advantageous for the research community to continue to identify these differences as they may illuminate the most effective way to address eating disorder symptoms and fears between individuals of different ages. What Mindful Eating is Really About By: Irina Vanzhula, B.A. People who come to my mindful eating workshop often say that they want to learn to eat healthier, lose weight, and reduce emotional and stress eating. I help them see that these goals have been imposed on them by society and the diet industry. I also challenge the idea that mindful eating is just another way to diet and then introduce a new way of thinking about their relationship with food. I usually see expressions of disbelief when I announce that emotional and stress eating are not their enemy. Dieting vs. Mindful Eating Any diet is by definition restrictive. Dieters deny themselves certain food groups, reduce how much they eat, or both. In addition to hunger, dieting creates a sense of deprivation, which in turn may make us sad or depressed. “I so much want that cupcake, but I can’t have it” (Johnson and Wardle, 2010). Some people may be able to convince themselves that they no longer like sweets and even override their hunger signals, but that takes a lot of mental energy and we can’t sustain it for a long time. Best-case scenario, we can maintain the eating pattern for a while using sheer willpower, but it eventually fails. Worst-case scenario dieting may trigger disordered eating (Stice, 2002) or even lead to weight gain over time. Cycles of Eating Many who attempt to forcefully regulate their eating get stuck in a cycle of dieting, overeating, and feeling guilty. Restricting our food intake overall and denying ourselves food we enjoy leads to hunger and intensified sense of craving. As a result, we may end up overeating and eating more of those foods we were trying to avoid in the first place. It is not all about willpower too, in fact, it has very little to do with willpower. When we are very hungry, our bodies are designed to crave fatty and sugary foods because it is a sure way to stock up on enough energy in case there is a shortage of food in the future again (Heshmat, 2011). Overeating is often associated with guilt or what we call “I have blown it” effect. We feel guilty for “breaking the rules” and decide to start all over tomorrow, and the cycle continues. Alternatively, overeating may make us feel depressed and bad about ourselves, which can trigger more emotional eating. 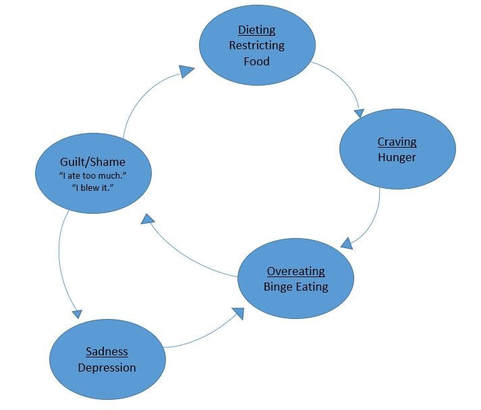 Automatic Pilot
What is the solution? In my workshop, I suggest that my participants abandon food rules and adopt a new set of goals: learn to eat intuitively by recognizing their hunger and fullness signals and satiate their body and mind. The key to achieving those goals is mindfulness. Mindfulness has many definitions and applications, but the one we focus on is awareness. Recent research is discovering that awareness may be the key to successful mindfulness-based interventions for disordered eating (Sala & Levinson, in press). Mindful awareness is paying attention to present moment experiences and is opposite of running on automatic pilot. Many of our eating experiences are indeed automatic. Our eating is a response to multiple environmental cues, such as smells, bowl of candy in the office, snacking while watching television, eating out of boredom or at the social event, and more. Overwhelmed by these stimuli, we lose touch with the true sensations of hunger and fullness, and true taste satisfaction. Hunger Practicing mindful awareness can help us disengage the automatic processes and really tune into our bodies. General meditation practice can help build the skill of paying attention, but mindful eating can be simply slowing down and paying attention to your meal. Next time you are about to eat, pause and take a breath. Notice how you are feeling and what you are thinking. Notice any attitude you have towards this meal you are about to eat. Notice the smell, the colors and shapes on your plate. Also notice sensations of your physical hunger. Hunger may feel different for each person, but in general we get hungry when our energy level is depleted and we need to refill our bodies. Physical hunger may be associated with lower blood sugar, fatigue, stomach empty and growling, and mouthwatering. This is how your body lets you know you need to eat, but how do we know when we are full? Fullness Most people see hunger and fullness as opposite ends of the same scale. If you are no longer hungry, you are full, and vice versa, right? In fact, body fullness and satiety are more complicated concepts. If you were to drink 20 oz of water, your stomach will feel very full, but you will likely still be hungry. Many people describe physical sensations of fullness as feeling bloated, having an extended stomach, feeling heavy, clothes getting tight, and even a lump in the throat. Have you ever eaten very fast when you are hungry and your stomach is full but you still feel hungry? These examples suggest that hunger and fullness are their own concepts and each can be measured on a separate scale. In general, physical hunger is about blood sugar levels, and physical fullness is about filling up the space of your stomach. Body Satiety Psychological hunger refers to wanting to eat for reasons such as boredom, sadness, food proximity, stress, and habit. You may snack at a party when you are not physically hungry or crave chocolate ice-cream at the end of a difficult day at work. Although we perceive emotional eating negatively, psychological hunger also needs to be satisfied. We call this body satiety. Consider this example: you eat a large portion of bland boiled chicken and rice. Your hunger is down, your fullness is up, but you are still craving dessert. That is because the meal did not satisfy you and you are still low on body satiety. Mindful eating proposes that instead of fighting these feelings, you satisfy them in a mindful way without overeating. What are you truly hungry for? The good news is that we don’t need to consume a lot of food to be satisfied. Out taste buds get tired very quickly: third, fourth and later bites won’t taste as good as the first one. This means, that we can satisfy that psychological hunger by having only a small amount of craved food. In addition, it is helpful to ask ourselves: what are we truly hungry for? If we are about to eat out of boredom, maybe we are really hungry for some good company and friendship? And last but not the least is self-compassion. If you do make a choice to satisfy your psychological hunger by eating our favorite food, don’t blame yourself. Be kind to yourself and recognize that this is what you need at that moment. Mindful eating introduces a completely different relationship with food and navigates you away from food rules. Mindful eating is based on building awareness of external and internal processes that dictate our eating behaviors. Developing eating awareness skills can help you end your battle with food and achieve your behavioral and health goals. To join our mindful eating group contact us here: http://www.louisvilleeatlab.com/eat.html To hear more about the negative impact of dieting, watch this TED talk: https://www.ted.com/talks/sandra_aamodt_why_dieting_doesn_t_usually_work From Media to Science: What Do We Get Wrong and Right about Men and Eating Disorders?
By Leigh C. Brosof For a long time, there was a belief in mainstream society that “boys don’t get eating disorders” and that eating disorders were a “girls’” issue. Fortunately, this view is changing with both research and the media becoming more inclusive in conversations around eating disorders. Researchers have shown that eating disorders and disordered eating are still highly prevalent among men. In fact, men suffer from some eating disorder symptoms (such as binge eating) just as much as women. While we are making great strides towards lessening the stigma around men and eating disorders, some misperceptions still abound, such as: 1) that you must be underweight to have an eating disorder, and 2) that there must be something “wrong” with men who get eating disorders. These misperceptions reflect general myths around eating disorders. Misperception 1: You must be underweight in order to have an eating disorder. Whereas this is untrue for every gender (eating disorders can affect individuals of any size!), it may make it particularly difficult for men to seek help, especially because symptoms such as binge eating, may not fit one’s “typical” view of an eating disorder. In addition, when men do start losing weight or become underweight, individuals may not think about an eating disorder as the problem. This misperception makes it more difficult for men to accept they have symptoms of an eating disorder or for medical professionals to spot these symptoms in men. Misperception 2: There is something “wrong” with men who get eating disorders. Despite societal stereotypes surrounding eating disorders, men are more similar than different in comparison to women when it comes to eating disorders. This means that there is a complex interplay of biological, psychological, and social factors that lead to the development of a disorder. Therefore, men’s eating disorder are not a “choice,” and it’s not anyone’s “fault” if they develop eating disorders. Rather, it is a serious mental health disorder. Men may also experience some types of eating disorder symptoms, such as muscle dysphoria, at higher rates than women. Muscle dysmorphia is when an individual has a drive to become more muscular and has insecurities around not being muscular enough. For men, this desire for muscularity may be coupled with a desire to be thinner or leaner. Men may also have concerns about different areas of their bodies than women. These similarities mean that, in general, treatments that have been developed for women should also work for men; however, it also means that certain aspects of these treatments should be tailored specifically for men. It’s also essential to remember that eating disorders affect people of ALL genders. In fact, some research suggests that individuals who are transgender or non-binary have eating disorders at higher rates than individuals who identify as cis-gender. Although the exact reason for this higher prevalence is not well-understood, it may have something to do with the stressors (and discrimination) that society puts on these individuals for not adhering to the gender binary. Research and treatments are slowly starting to include not only males, but also individuals of all genders; however, more effort still needs to be devoted in order to best serve individuals across the gender spectrum. For instance, right now, a comprehensive assessment of gender identity does not exist – something that our lab is trying to change. The most important thing that society and research can do is to acknowledge that eating disorders do not discriminate – we need to include individuals of all genders in the conversation to decrease stigma and increase the likelihood that men and individuals of other genders will seek treatment. If you are a man who is suffering from an eating disorder, to learn more about men and eating disorders or for resources for treatment: http://namedinc.org/  Reflections from the NEDA walk
By: Cheri A. Levinson, Ph.D. I was fortunate to join over 200 fellow walkers on Saturday to fight against eating disorders and bring awareness to the psychiatric disorder with the highest rates of mortality. I left the walk feeling extremely inspired. Inspired to continue the hard work that my team at the University of Louisville (www.louisvilleeatlab.com) and at the Behavioral Wellness Clinic (http://bewellproviders.com/) spend our lives on. Perhaps the most inspiring part of the walk was the community of people coming together showing our state and the city of Louisville how many people are impacted and that we are not alone. As I said in my speech (read full transcript here) ‘…every day I have conversations with people, many of you who are here, many who are across the globe, but all who care about changing society and the treatment of EDs for the better. This inspires me.’ It was inspirational to see so many people come together to bring about change. It made me feel not alone, as I am sure it did to most all who attended the walk. But I also left the walk feeling that a few messages still need to be communicated. A WDRB article (http://www.wdrb.com/story/36382951/hundreds-take-part-in-walk-at-bellarmine-university-to-raise-awareness-of-eating-disorders) covered the walk and highlighted two points. First, more treatment centers are needed locally. Second, there is very little research funding allocated to eating disorders. These messages need to be out there. But I also think that a word of caution is needed when putting these messages to the public. More treatment centers are needed locally. Yes! This is a given. Our community needs a treatment center. We are a city of 1 million people, meaning at least 70,000 people in our community have an eating disorder. We need more access to empirically-validated treatments in Louisville. Key words here are empirically-validated treatments. We need to be careful about recruiting an eating disorder center to our community. Treatment centers vary in the quality of treatment provided. I can say from experience (and from research) that there is often a huge gap in the type of treatment that is provided and the type of treatment that *could* be provided. We need a treatment center in Louisville, but we need more than a ‘status quo’ treatment center that will provide sub-optimal care. More funding for research is needed. Figures from the National Institute of Health show a huge discrepancy in the funding allocated to eating disorders versus other mental and physical health problems given the societal and personal costs. In plain language, research in the eating disorders is extremely underfunded. I am in the process of applying for three national grants. Two from NEDA and one from the National Institute of Health that would establish UofL as the primary site in a network of seven treatment development centers. In my opinion (which is of course, obviously biased) these grants hold the power to transform eating disorder treatment. Unfortunately, the stark reality is that the likelihood of receiving these grants are low, not because they shouldn’t be funded, but because there are not enough research dollars. I do not see either of these issues as separable. The ideal treatment center is grounded in research and good research that has real impact is grounded in actual treatment. We stand at the cusp of an opportunity to create a world-renowned, state of the art, treatment, research, and training facility right here in Louisville that will provide treatment, development of novel treatments, and training, that our state (and nation) desperately needs. We are working hard at UofL and at the Behavioral Wellness Clinic to make these goals happen, but the more support, both financial and physical we receive, (which can only happen through awareness) the faster we can make this a reality, so that we can decrease the extreme amount of suffering and impairment that eating disorders cause. Anorexia Nervosa in Russia
By: Irina Vanzhula I grew up in the city of Saint-Petersburg, Russia and moved to the United States 10 years ago. I have noticed many differences, including how women’s sizes are perceived in each country. A woman wearing dress size 8-10 in the US would be considered by most to be of normal weight, but in Russia, she would be called overweight. Most clothing stores do not even carry sizes higher than 10, and Plus size starts with 12. The “normal” clothing size in Russia is 0-4, and women go to considerable lengths to obtain this size at all costs. The thin-ideal is pervasive in Russian culture with its famous ballerinas and supermodels. My 14-year old brother Vasya is a student at the world famous Vaganova Academy of Russian Ballet. He spends about 6 out of his 12-hour day dancing and only eats once a day. He is underweight, but is repeatedly told that if he gains weight he will be kicked out of the Academy. Vasya is not the only one. Although media’s focus on thin bodies is ubiquitous across countries, Russian women experience additional pressures to look “perfect.” Russia has approximately 85 men for 100 women, and considering very high rates of substance abuse in men, the number of ‘quality bachelors’ is even lower. To be competitive, Russian women pay extreme attention to their looks, including body weight and shape. It is considered necessary to dress up and do hair and make-up just to go to a grocery store, and wearing sweatpants in public is unthinkable. Much of woman’s value is based on looks, and being thin is a sign of having strong willpower and being successful. Based on these observations, I suspect that prevalence of eating disorders and especially anorexia nervosa (AN) in Russia would be higher than in the US. Thus, I decided to do some research. My search revealed that no epidemiological studies have been done and no official statistic of eating disorders exists in Russia. Prevalence rates reported range from 0.5% (Bobrov, 2015) to 20% (Anorexia in Russia, n.d.). Since Russians don’t believe in mental illness and most people don’t seek treatment, the rates are likely underreported. A large population with subclinical AN symptoms may account for the large discrepancy in prevalence rates. I continued my search to uncover how AN is portrayed in both internet and the scientific community. Most internet articles accurately described the disorder and emphasized fear of fat, perfectionism, and disturbed body image. Health complications were usually mentioned, but I did not find anything about high levels of suicide, which is likely due to the topic of suicide being a social taboo in Russia. One disturbing discovery was that the webpages that described the dangers of AN were full of advertisements of various diets. For example, next to the article “Anorexia – severe disease statistics” you can find “how to lose weight and keep it off forever” and advertisements of various diets (www.http://www.on-diet.ru). Most internet articles recommended the help of a professional, but after reviewing treatment options, I lost most of my optimism. I did not find any specialized eating disorder clinics in the entire country, and help with AN was offered at general medical or psychiatric hospitals. One gastrointestinal clinic advertised AN treatment, but the treatment team consisted most of the dietitians and only one psychologist. Even the clinics that offer any kind of treatment for eating disorders are few and spread thin. Most clinics are located in Moscow and Saint-Petersburg. Considering size and population of the country, the majority of Russians don’t have access to any eating disorder treatment or even a therapist. Thousands of small Russian towns are lucky to have one general practitioner, and the closest psychologist is usually hundreds of miles away. Next, I turned to scientific journals. Most of the information was consistent with that in US journals. I came across one surprising trend strongly linking AN with psychotic disorders. Bobrov (2015) describes AN as having inaccurate cognitive perceptions of reality and empathizes its high comorbidity with schizophrenia. Further, Artemyev & Vasiliev (2012) explain that some researchers see AN as a schizophrenia syndrome, citing an article from 1932, and report that schizophrenia precedes AN in 25% cases. In another study, out of 101 women with AN on inpatient psychiatric unit, 81 were diagnosed with schizophrenia (Artemyeva & Arsenyev, 2010). Patients with AN often report that their family and friends find their eating disorder related beliefs strange and unusual, and refusing to eat despite life-threatening complications may be perceived as particularly strange. This interpretation may have led to over-diagnosis of schizophrenia in those with AN. However, recent studies report that prevalence of psychotic in those with AN is no higher than in general population (Seeman, 2014). Russian psychologists, however, may still over-diagnose schizophrenia, or these statistics are a result of a biased sample. They mostly studied patients in psychiatric hospitals, where comorbidity of severe mental disorders is high. On the other hand, new research revealed a genetic link between AN and psychosis (Duncan et al., 2017), so there may be some connection there after all. One major implication of connecting AN with schizophrenia in the literature is increased stigma. If seeking treatment for AN means the high probability of being diagnosed with a psychotic disorder and likely prescribed anti-psychotic medication, it is not surprising that people would avoid it at all costs. In conclusion, the amount of social pressure on all Russian women to be thin is incredible, and the standards are impossible to achieve. People who have symptoms of AN are admired and praised for their strong wills and dedication. The scientific community is lagging behind in proper diagnosis and further contributes to already high stigma of mental illness. Although rates of AN may be high in Russia, treatment options are almost non-existent. Epidemiological studies that bring attention to prevalence of AN in Russia and lack of treatment options are needed. While the research field is catching up, all of us can help increase awareness by making translated US articles available on the Russian web. |
Archives
January 2024
Categories |
- About
- People
- Our Research & Publications
-
Participate in Research
- Personalized Interventions and Outcomes: Navigating Eating Disorder Experiences and Recovery (PIONEER) Study (Online)
- Tracking Restriction, Affect and Cognitions (TRAC) Study (Online)
- Virtual Reality Study
- Facing Eating Disorder Fears Study (Online)
- Personalized Treatment and CBT-E Study (Online)
- Body Project Summer Camp
- The Body Project
- Clinical Screener Study (Online)
- Clinic, Supervision, and Consultation
- Blog & In the Press
-
Archived Studies
- Predicting Recovery Study (Online)
- Online Single Session Resources
- Reconnecting to Internal Sensations and Experiences (RISE) Study
- Web-Based Mindfulness Study
- Personalized Treatment Study
- Online Imaginal Exposure Study
- In-Vivo Imaginal Exposure Study
- Daily Habits 3 Study
- Daily Mood Study
- COVID-19 Daily Impact Study
- Conquering fear foods study
- Louisville Pregnancy Study
- Approach and Avoidance in AN (AAA) Study
- Web-Based Mindfulness for AN & BN Study
- Barriers to Treatment Access (BTA) Study!
- Mindful Self-Compassion Study
- Network EMA Study
- Legacy of Hope Summit Report
- DONATE-CURE EATING DISORDERS!
- Directions
- Statistical Consultation
- About
- People
- Our Research & Publications
-
Participate in Research
- Personalized Interventions and Outcomes: Navigating Eating Disorder Experiences and Recovery (PIONEER) Study (Online)
- Tracking Restriction, Affect and Cognitions (TRAC) Study (Online)
- Virtual Reality Study
- Facing Eating Disorder Fears Study (Online)
- Personalized Treatment and CBT-E Study (Online)
- Body Project Summer Camp
- The Body Project
- Clinical Screener Study (Online)
- Clinic, Supervision, and Consultation
- Blog & In the Press
-
Archived Studies
- Predicting Recovery Study (Online)
- Online Single Session Resources
- Reconnecting to Internal Sensations and Experiences (RISE) Study
- Web-Based Mindfulness Study
- Personalized Treatment Study
- Online Imaginal Exposure Study
- In-Vivo Imaginal Exposure Study
- Daily Habits 3 Study
- Daily Mood Study
- COVID-19 Daily Impact Study
- Conquering fear foods study
- Louisville Pregnancy Study
- Approach and Avoidance in AN (AAA) Study
- Web-Based Mindfulness for AN & BN Study
- Barriers to Treatment Access (BTA) Study!
- Mindful Self-Compassion Study
- Network EMA Study
- Legacy of Hope Summit Report
- DONATE-CURE EATING DISORDERS!
- Directions
- Statistical Consultation
 RSS Feed
RSS Feed